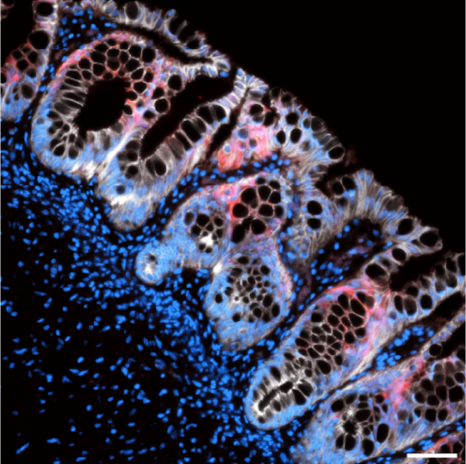
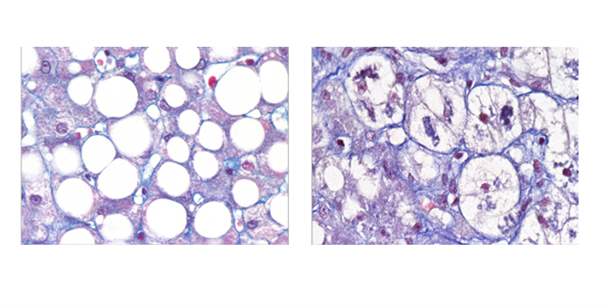
 Histological cross-section of a human colonic organoid generated in a confined culture system and following transplantation (blue: cell nuclei; white: intestinal epithelium; red: colonic enzyme) © Maxime Mahé/Inserm. CC-BY 4.0 International license
Histological cross-section of a human colonic organoid generated in a confined culture system and following transplantation (blue: cell nuclei; white: intestinal epithelium; red: colonic enzyme) © Maxime Mahé/Inserm. CC-BY 4.0 International license
More and more people are suffering from gastrointestinal diseases. To better understand these conditions and provide solutions for patients, scientists are working on organoids, small three-dimensional biological structures capable of replicating certain functions of an organ. These models are valuable tools for studying cell development and disease mechanisms. A team from Inserm and the University of Nantes, in collaboration with American teams [1], has developed a new culture method that, for the first time, enables the production of large, functional human intestinal organoids and does so twice as fast as existing methods. Furthermore, these organoids can develop their own nerve cells. This breakthrough offers new prospects for the study of gastrointestinal diseases and the development of future therapeutic applications. These results were published in the journal Nature biomedical engineering.
Organoids are three-dimensional biological structures created from stem cells that are capable of multiplying indefinitely (or nearly so) and giving rise to cells with specific functions. Researchers have been studying them for about fifteen years, with the initial goal of understanding the processes involved in the development and anatomical organization of our tissues. Today, organoids have become excellent tools for biomedical research.
Cultured in vitro, the cells organize and specialize through processes similar to those observed during embryonic development. They thus form organoids that replicate certain structural and functional characteristics of the tissues or organs from which they originate.
Until now, however, the culture methods used to produce organoids had several limitations. They did not perfectly replicate the conditions of embryonic development in vitro and required transplantation into an animal model to reach a more advanced developmental stage.
The team led by Maxime Mahé, an Inserm researcher at the Enteric Nervous System in Digestive and Brain Diseases laboratory (TENS – Inserm/Nantes University), sought a way to improve tissue generation while simplifying existing methods.
The scientists have developed a new method for culturing intestinal organoids called the confined culture system (CCS), which is based on 3D printing technology. This technique creates an environment conducive to the growth and cellular differentiation of organoids.
The results show that after 14 days of culture in this specific environment (see box below), the organoid structures produced all cell types and structures that previously took 28 days to form. Once transplanted into a mouse model (to allow the organoids to complete their cellular development), the scientists observed that the organoids adapted to the host’s physiology, along with improved tissue growth and overall development.
The confined culture system uses 3D printing technology to create tray-shaped molds from surgical resin, then fills these molds with degassed polydimethylsiloxane—a type of flexible, rubber-like silicone.
These new trays feature grooves designed to confine a set of spherical organoids in a single row, thereby promoting their fusion and maturation (a 3D cell culture model). These fusions occur within a special mixture of nutrients and other ingredients that support the initial growth of stem cells into more complex organoids.
By day six, the distinct spheroids develop into unified structures along the grooves of the plates. These are then transferred to a hydrogel to continue growing for an additional eight days.
By day fourteen, the organoid structures have produced all cell types and structures that previously took 28 days to form.
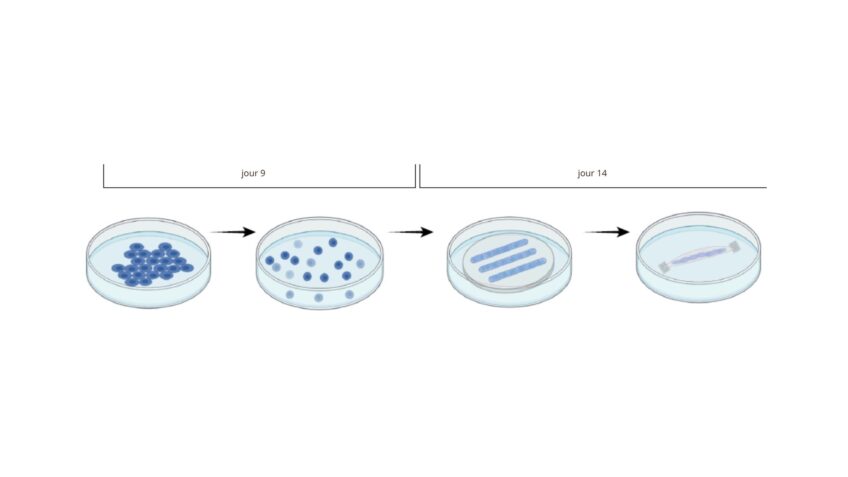 Schematic diagram of the confined cultivation system. © BioRender; Poling, H.
Schematic diagram of the confined cultivation system. © BioRender; Poling, H.
In addition to being a faster method, this new confined culture system has made it possible to create small intestine, colon, and stomach organoids nearly 10 times larger than those obtained using previous methods. Whereas organoids previously measured 1 cm, the new ones can reach 8 cm.
Unlike previous methods, this confined culture system allows the organoids to spontaneously develop an enteric nervous system (which regulates digestive functions). Even before transplantation, researchers observed that this nervous system was functional, capable of responding to stimuli and exhibiting neuronal activity.
“Our work shows that we are now able not only to generate larger, complex gastrointestinal organoids, but also ones equipped with an enteric nervous system,” explains Maxime Mahé, the study’s last author.
“This culture method could help accelerate the production of tissues derived from fairly large organoids that can be used in regenerative medicine or for transplanting the small intestine, stomach, or colon in patients. Such tissues would also be valuable for future studies on digestive diseases such as Hirschsprung’s disease, as well as for more accurately assessing the risks of organ damage associated with taking oral medications,” notes Maxime Mahé.
[1] This study was conducted in collaboration with, among others, Cincinnati Children’s Hospital Medical Center (CCHMC)








 © Adobe stock
© Adobe stock