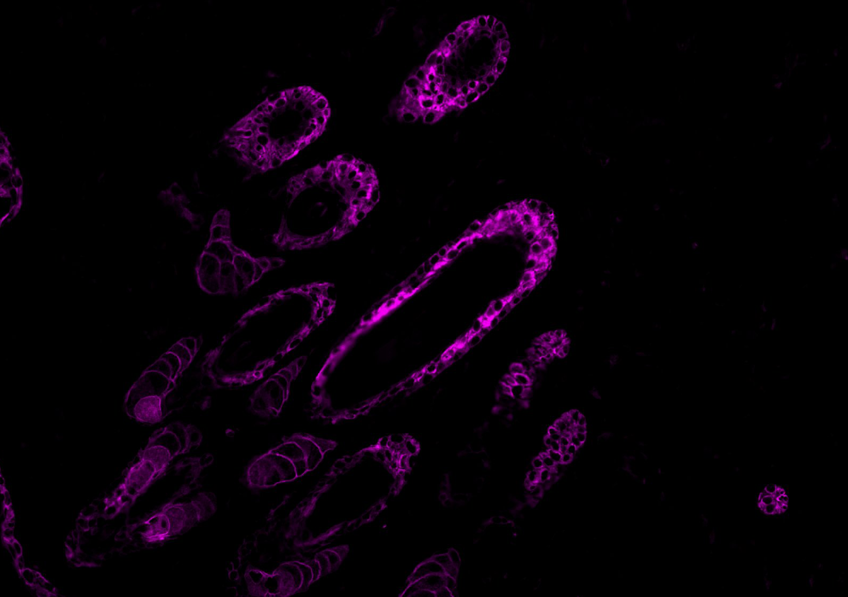
 Co-marquage insuline (vert)/glucagon (rouge) et noyaux (bleu) © Guillaume Canaud et Sophia Ladraa – Institut Necker-Enfants Malades (Université Paris Cité, AP-HP, Inserm)
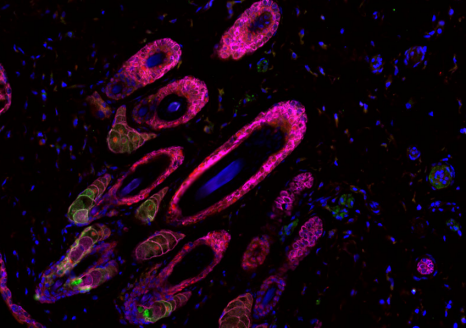
Co-marquage insuline (vert)/glucagon (rouge) et noyaux (bleu) © Guillaume Canaud et Sophia Ladraa – Institut Necker-Enfants Malades (Université Paris Cité, AP-HP, Inserm)
Four years after receiving approval from the US Food and Drug Administration (FDA), alpelisib has now been approved by the European Medicines Agency for the treatment of severe forms of PIK3CA-related overgrowth spectrum (PROS), including CLOVES syndrome. This therapeutic breakthrough is the result of the work carried out by Professor Guillaume Canaud and his team within the Translational Medicine and Targeted Therapies Unit at Université Paris Cité, Necker-Enfants Malades Hospital AP-HP, and Inserm.
This European marketing authorisation marks a major milestone for patients with PIK3CA-related overgrowth spectrum (PROS), a group of rare genetic disorders responsible for complex and sometimes severe malformations. It is based on nearly ten years of translational research conducted at Université Paris Cité, Necker-Enfants Malades Hospital (AP-HP), and Inserm, leading to the identification, assessment, and validation of a new therapeutic strategy targeting the PIK3CA gene.
A rare disease with no treatment until now
Patients with syndromes caused by PIK3CA mutations arising during embryonic development, including CLOVES syndrome, one of the most severe forms, experience major deformities and vascular abnormalities.
In the most severe cases, patients develop abnormal fatty tissue overgrowth, vascular malformations, scoliosis, significant skeletal involvement, and deformities affecting various organs, including the brain and kidneys.
Until recently, no curative treatment was available for these patients, whose prognosis could be life-threatening in the short or medium term. They had to rely on symptomatic treatments, repeated embolisation procedures, or major surgery to preserve healthy organs or limbs.
Ten years of research, from bench to bedside
Originally developed to treat breast cancer, alpelisib was identified by Professor Guillaume Canaud’s team as a potential treatment for patients with PROS. Between 2016 and 2018, the team developed preclinical models reproducing the symptoms and deformities associated with these syndromes and demonstrated the effectiveness of this therapeutic strategy before evaluating it in patients.
This work led to the first marketing authorisation for alpelisib in this indication in the United States in April 2022. Since then, the number of treated patients has continued to grow, and the data accumulated to date confirm the treatment’s lasting efficacy.
Particularly encouraging long-term results
The European authorisation, granted four years after the drug was first approved in the United States, is based in particular on the results of the international EPIK-P3 study, presented at the 2026 International Society for the Study of Vascular Anomalies (ISSVA) congress in Philadelphia.
This prospective study assessed the long-term effects of alpelisib in patients with PROS. After an average follow-up period of seven and a half years, the results showed excellent treatment adherence, with 97.5% of patients still receiving therapy. Side effects were mainly moderate and well controlled, while efficacy was confirmed and increased over time, with progressive improvement in symptoms and a reduction in disease-related malformations.
For some patients, the benefits observed were remarkable. Young patients who had lost the ability to walk regained their mobility, while others partially recovered sensory functions such as sight and hearing that had been impaired by the disease.
European recognition for research conducted in France
This major therapeutic advance has now been recognised by the awarding of the Mendel Medal to Professor Guillaume Canaud. Awarded annually by the European Society of Human Genetics (ESHG), the medal is one of the most prestigious distinctions in the field of genetics. It honours researchers whose work has profoundly transformed the understanding or treatment of genetic diseases.
On 16 June 2026, Professor Guillaume Canaud became only the second French scientist to receive this distinction, after Professor Emmanuelle Charpentier, who was honoured in 2018 for her pioneering work on CRISPR-Cas9 technology.
This award recognises the full body of work that led to the identification of alpelisib as a treatment for PIK3CA-related genetic diseases, from the understanding of the underlying biological mechanisms to its clinical development and regulatory approval.
“The Mendel Medal is a tremendous source of pride for all the research and care teams involved in this journey. It recognises a collective effort led in France, made possible by the combined commitment of scientists, clinicians, patient organisations, and all our partners.”
Following this European authorisation, although the drug is already available in France, alpelisib must now be assessed by the French National Authority for Health (HAS) to determine reimbursement conditions and enable the widest possible access for patients in France. At the same time, research is continuing to evaluate the benefits of the treatment in less severe forms of the disease and to further improve care for patients with PIK3CA-related syndromes.

 Molecules passing through the colon epithelium via specialized pathways (goblet cells). In red: the molecules transported (antigens); in blue: the epithelium. © Institut Pasteur/Microbiome-Host Interactions/Clara Delaroque and Benoit Chassaing
Molecules passing through the colon epithelium via specialized pathways (goblet cells). In red: the molecules transported (antigens); in blue: the epithelium. © Institut Pasteur/Microbiome-Host Interactions/Clara Delaroque and Benoit Chassaing
 Mouse skin structure after stretching, using histological staining. The scale bar corresponds to 100 micrometers. © Darawan Tabtim-On and Renaud Leclère – Experimental Pathology Platform, Institut Curie
Mouse skin structure after stretching, using histological staining. The scale bar corresponds to 100 micrometers. © Darawan Tabtim-On and Renaud Leclère – Experimental Pathology Platform, Institut Curie