This colorized electron microscope image shows SARS-CoV-2 isolated from a patient in the USA. Viral particles emerge from the surface of the laboratory-cultivated cells. © NIAID-RML Creative Commons.
Why are children less susceptible than adults to critical forms of COVID-19? This question has been studied by many scientists since the pandemic began. A number of interesting avenues are emerging, notably suggesting differences in immune response following SARS-CoV-2 infection. In a new study, researchers from Inserm, Université d’Angers and Angers University Hospital, members or partners of the Regional Center for Research in Cancerology and Immunology Nantes-Angers (CRCINA) have shown that the interferon response, which is part of the innate immune response, differs according to the age of the patient. Their findings have been published in Frontiers in Immunology in November 2021.
The symptoms of COVID-19 vary widely from one person to another. While some are asymptomatic following SARS-CoV-2 infection, others develop severe and possibly fatal forms of the disease. Since the start of the pandemic, age has been identified as a major risk factor for developing a severe form of COVID-19. Unlike adults, and especially the elderly who are very vulnerable to infection, children usually have no clinical signs of the disease (or only mild symptoms).
Numerous research teams are trying to identify the immune response parameters that could explain this difference in susceptibility between young and elderly people.
In this collaborative research, scientists from Inserm and Université d’Angers at the Regional Center for Research in Cancerology and Immunology Nantes-Angers, as well as the Virology and Immunology laboratories at Angers University Hospital, have hypothesized that children are protected due to a stronger local innate immune response, in the nasopharyngeal mucosa. So far, there has been less research into innate immunity to COVID-19 than into adaptive immune response[1].
A closer look at immune response
Innate immunity is the immediate response that occurs locally, at the point of entry of a pathogenic microorganism, in any individual – even in the absence of prior contact with that microorganism. It is the first barrier of defense against pathogens. In the event of a viral infection, it primarily deploys Natural Killer cells
that kill the cells infected with a virus. It also induces the production of interferons by the infected cells, and it is these interferons that protect the adjacent cells from infection.
Adaptive immunity is a response that takes 5 to 7 days to become protective when the pathogen is encountered for the first time (primo-infection), but is more rapidly effective once the pathogen has already been encountered (this is known as a memory response). In the event of a viral infection, it deploys two types of protective immune cells: antibody-producing B cells that bind to the virus and “neutralize” it, namely by preventing it from entering the cells and by promoting its elimination, and cytotoxic CD8+ T cells that kill the infected cells. The B and T cells recognize protein structures (of the virus) known as antigens.
Following infection with a virus or vaccination, the level of antibodies and lymphocytes recognizing the virus decreases over time. Nevertheless, the so-called “memory” B and T cells remain in the body and keep watch, acting faster and more efficiently if they encounter the same virus in the future.
Different interferon responses
In their research, the scientists analyzed nasopharyngeal samples from 226 people who had come for a PCR test at a drive-through screening center at Angers University Hospital between March 2020 and March 2021. Of these individuals, 147 were infected with SARS-CoV-2. “Our research was original in that we had not preselected the participants, so as not to bias the results, and also that we were interested in innate immunity – and more specifically the interferon response,” emphasizes Yves Delneste, an Inserm researcher who took part in this study.
When cells are infected with any given virus, they rapidly produce type I (IFN-α/β) and type III (IFN-l) interferons, which are powerful natural antiviral molecules. They are called interferons because they “interfere” with the replication of the virus and protect the adjacent cells from infection.
While these interferons all have antiviral activity, their modes of action are not redundant. Each induces an antiviral response of a different intensity and duration and has a different but complementary action on immune response[2].
An inadequate or inappropriate interferon response will not make it possible to contain the replication of the virus or it may promote a pathological immune response (for example, an exacerbation of the immune system as seen with severe forms of COVID-19).
Analysis of the samples studied by the research team revealed that in subjects infected with SARS-CoV-2, the expression profiles of type I (IFN-α/β) and type III (IFN-l) interferons differ with age. Thus, children under 15 years of age have an increased expression of type III interferons, locally-acting molecules with limited inflammatory properties, which control the virus locally at its entry point in the nasopharyngeal mucosa. Conversely, adults, especially elderly adults, preferentially express type I interferons, which are inflammatory and have a more systemic action (in the whole body).
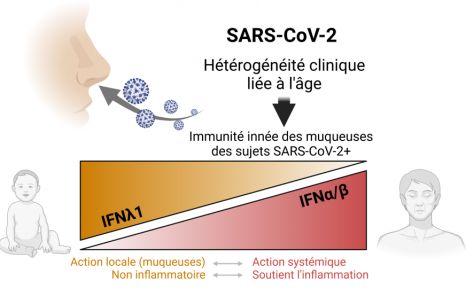
“These findings help to explain why children are less susceptible to critical forms of COVID-19 than adults. Type III interferons, which primarily act by protecting the epithelium at local level, could control infection at the point of entry, without inducing excessive widespread inflammation, thereby preventing the slide towards the inflammatory storm with mass cell destruction that is seen in severe forms,” emphasize Pascale Jeannin (university professor and hospital practitioner) and Dominique Couez (university professor) in Angers, who led this research.
Based on these findings, the scientists will now conduct a prospective study to evaluate whether, in children with clinical signs of the disease, the characteristics of the interferon response associated with severe forms in adults are present and whether they can predict the course of infection.
1 see text box on innate and adaptive immunity
2 see text box
These contents could be interesting :
Medias
Sources
Age-Related Expression of IFN-l1 Versus IFN-I and Beta-Defensins in the Nasopharynx of SARS-CoV-2-Infected Individuals
Charly Gilbert1,2, Caroline Lefeuvre3,4, Laurence Preisser1, Adeline Pivert3,4, Raffaella Soleti1, Simon Blanchard1,2, Yves Delneste1,2, Alexandra Ducancelle3,4, Dominique Couez1† and Pascale Jeannin1,2*†
1 Univ Angers, Université de Nantes, CHU Angers, Inserm, CRCINA, SFR ICAT, Angers, France,
2 Laboratory of Immunology and Allergology, Angers University Hospital, Angers, France
3 Laboratory of Virology, Angers University Hospital, Angers, France
4 Université d’Angers, CHU Angers, HIFIH, SFR ICAT, Angers, France
Frontiers in Immunology, Novembre 2021