
Researcher Contact
Jérôme Estaquier
Inserm researcher
Unit 1124 Environmental Toxicology, Therapeutic Targets, Cell Signalling and Biomarkers (Inserm/Université Paris Cité)
Email: rf.setracsedsirap@reiuqatse.emorej

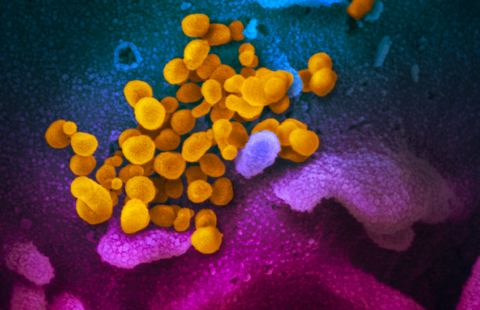
This transmission electron microscope image shows SARS-CoV-2, isolated from a patient in the U.S., emerging from the surface of cells cultivated in a laboratory. © National Institute of Allergy and Infectious Diseases-Rocky Mountain Laboratories, NIH. Public domain.
Several months after infection with SARS-CoV-2, some patients still have symptoms: a phenomenon commonly referred to as “long COVID”. In new research, teams from Inserm and Université Paris Cité[1], in collaboration with the University of Minho in Braga (Portugal), have shown that this could be explained biologically by abnormalities of the immune system associated with the persistence of the virus in the mucous membranes. These findings, published in Nature Communication, could in the longer term pave the way for a diagnostic tool for long COVID.
Despite the fact that various studies consider long COVID to affect between 10 and 30% of people infected with SARS-CoV-2, its diagnosis and treatment remain difficult. The team of Inserm researcher Jérôme Estaquier, in collaboration with that of Ricardo Silvestre at University of Minho in Portugal, is conducting research to explain this phenomenon from the biological point of view.
At the present time, few biological criteria, apart from the persistence of symptoms beyond three months after the acute infection, enable its diagnosis. Once a patient is not fully recovered after this period, they are considered to have long COVID. Without a more reliable means of diagnosis, it is difficult to offer the appropriate care.
In order to better understand long COVID and find diagnostic markers, the researchers studied the immune systems of 164 people six months after they were infected. They analysed the blood samples of 127 people, half of whom with long COVID (fatigue, shortness of breath, cough, muscle or chest pain, anxiety, etc.) and those of 37 controls who had not been infected.
The researchers focused on certain immune cells, namely the T cells (including CD8 cells) involved in eliminating the virus, and the SARS-CoV-2 antibodies. In addition, they had blood samples that were taken during the acute phase of the disease for 72 of these patients, enabling them to retrospectively compare the level of inflammation at the early stage in those who went on to develop long COVID or not.
Several immune markers identified
The researchers identified a number of blood markers present six months after infection in 70-80% of the subjects with long COVID, while those same markers were rare in the subjects who had not developed it.
In particular, the teams showed that a CD8 cell subtype expressing the inflammatory protein granzyme A is present in excess, whereas another CD8 subtype, this time expressing integrin b7, is present in small quantities. Yet it is the latter subpopulation that is essential for controlling viruses in the mucous membranes. In addition, virus-specific IgA antibodies are also present in excess whereas they should be rapidly eliminated if the virus is absent. These observations suggest the persistence of the virus in the body and especially in the mucous membranes.
The researchers hypothesise that SARS-CoV-2 could make itself at home in the intestinal mucosa as it is more “permissive” in immune terms than the rest of the body, insofar as the virus has to tolerate the bacterial flora. Other viruses, such as HIV, also use this escape strategy. Initially present in the lung mucosa, SARS-Cov-2 could therefore descend to the intestine and persist there without the immune system being able to eliminate it completely.
In the final stage of the study, when evaluating the initial level of inflammation during the acute phase, the scientists observed an association between an inflammatory response characterized particularly by very high levels of interferon IP-10 or interleukin IL-6 and the risk of going on to develop long COVID.
“This confirms clinical observations that the initial severity of COVID is associated with a higher risk of developing long COVID,” specify the researchers. “One hypothesis is that people with more exacerbated early immunodeficiency develop more severe initial forms of COVID-19 and fail to effectively eliminate the virus that passes into the intestinal mucosa, where it settles for a long time. The immune system kind of ends up tolerating it at the cost of persistent symptoms of varying intensity and nature,” explains Estaquier.
The objective is now to validate these findings in new cohorts to determine whether some of these markers could be used as a diagnostic tool.
“If measuring IgA some time after the acute phase and potentially CD8 b7 cells was able to diagnose long COVID, doctors could make an objective diagnosis. Then we could think about therapeutic targets based on this research,” concludes Estaquier.
[1]This research in France was supported by the Fondation pour la Recherche Médicale, the French National Research Agency (ANR), and ANRS | Emerging Infectious Diseases.
Jérôme Estaquier
Inserm researcher
Unit 1124 Environmental Toxicology, Therapeutic Targets, Cell Signalling and Biomarkers (Inserm/Université Paris Cité)
Email: rf.setracsedsirap@reiuqatse.emorej
Post-acute sequelae of COVID-19 is characterized by diminished peripheral CD8+β7 integrin+ T cells and anti-SARS-CoV-2 IgA response
André Santa Cruz # 1 2 3 4, Ana Mendes-Frias # 5 6, Marne Azarias-da-Silva 7, Sónia André 7, Ana Isabel Oliveira 8, Olga Pires 8, Marta Mendes 8, Bárbara Oliveira 8, Marta Braga 8, Joana Rita Lopes 8, Rui Domingues 8, Ricardo Costa 8, Luís Neves Silva 8, Ana Rita Matos 8, Cristina Ângela 8, Patrício Costa 5 6, Alexandre Carvalho 5 6 8 9, Carlos Capela 5 6 8 9, Jorge Pedrosa 5 6, António Gil Castro 5 6, Jérôme Estaquier 10 11, Ricardo Silvestre 12 13
1Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal.
2ICVS/3B’s – PT Government Associate Laboratory, Braga/Guimarães, Portugal.
3Department of Internal Medicine, Hospital of Braga, Braga, Portugal. tp.ohnimu.dem@oaojcserdna.
4Clinical Academic Center-Braga, Braga, Portugal. tp.ohnimu.dem@oaojcserdna.
5Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal.
6ICVS/3B’s – PT Government Associate Laboratory, Braga/Guimarães, Portugal.
7INSERM-U1124, Université Paris Cité, Paris, France.
8Department of Internal Medicine, Hospital of Braga, Braga, Portugal.
9Clinical Academic Center-Braga, Braga, Portugal.
10INSERM-U1124, Université Paris Cité, Paris, France.
11CHU de Québec – Université Laval Research Center, Québec City, Québec, Canada. rf.oohay@reiuqatse.
12Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal. tp.ohnimu.dem@ertsevlisodracir.
13ICVS/3B’s – PT Government Associate Laboratory, Braga/Guimarães, Portugal. tp.ohnimu.dem@ertsevlisodracir.
#Contributed equally
Nature Communications, avril 2023
DOI : 10.1038/s41467-023-37368-1