According to the results of an IFOP survey, “Les Français et les Rhumatismes” (Rheumatic Diseases and the French), conducted by Inserm and “Ensemble Contre les Rhumatismes” (Together Against Rheumatic Diseases), 93% of French people report having already suffered from joint pain[1] and one in two were suffering from it at the time of responding to the survey. This joint pain strongly affects their daily life. Quality of sleep and the ability to perform leisure activities are the two aspects of daily life that are most affected, ahead of working life and family life.
The results of this survey emphasise the need to continue to conduct ambitious research programmes to find new treatments, and encourage the French to act from the earliest age possible to retain their “joint capital.”
This press file has been prepared to mark World Arthritis Day and the French initiative “Ensemble Contre les Rhumatismes” (ECR, Together Against Rheumatic Diseases) which will take place on 12 October next.
ECR brings together the 3 most important contributors to research on joint diseases in France. Created at the initiative of the National Alliance for Life Sciences and Health (Inserm-AVIESAN), Fondation Arthritis and the French Society for Rheumatology (SFR), Ensemble Contre les Rhumatismes (ECR, Together Against Rheumatic Diseases) has the mission of promoting research in Rheumatology in order to prevent, relieve and cure diseases of the bones and joints, which affect one quarter of the European population.
Rheumatic diseases
Rheumatic diseases comprise all diseases of the musculoskeletal system (bones / cartilages / muscles tendons / ligaments).
Osteoarthritis and Arthritis are multigenerational diseases that affect the young and less young.
Rheumatoid Arthritis and Ankylosing Spondylitis are the most common inflammatory rheumatic diseases.
12-13 million French people suffer from rheumatic diseases including:
9-10 million from osteoarthritis
600,000 from chronic inflammatory rheumatic diseases (rheumatoid arthritis, spondylitis)
4,000 children suffer from idiopathic juvenile arthritis, a serious form of juvenile arthritis
True / False
Joint pain affects only a small part of the population / FALSE
More than 1 in 2 French people presently suffer from joint or bone pain
1/3 of 18-24 year olds presently suffer from joint pain*
WHO has declared lumbago to be the leading cause of disability worldwide? In France nearly 4,000 children suffer from inflammatory rheumatic diseases, nearly 600,000 adults suffer from the same diseases, and nearly 10 million French people suffer from osteoarthritis. These diseases are therefore clearly not only due to the ageing population.
Joint diseases are not serious / FALSE
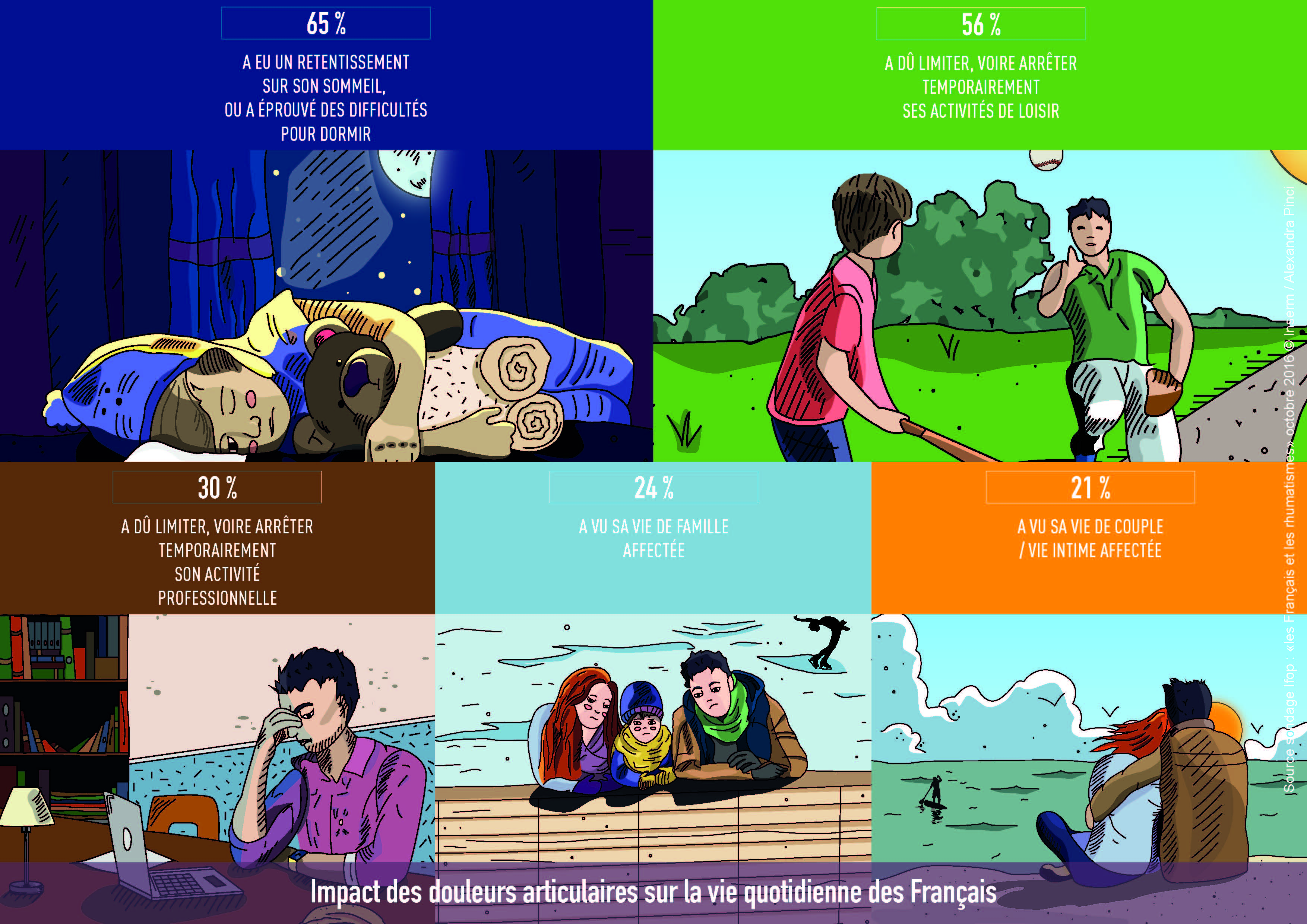
65% of French people have had their sleep affected by joint pain.
Of those under 25 years of age, more than 1 in 2 young people consider rheumatism to have had an impact on their social and family life*
Joint diseases have a major impact on quality of life and sleep, but also on mortality. They are the main reason for sick leave. Rheumatic diseases are the leading cause of chronic pain. They have a direct impact on mobility and an indirect impact by increasing the risk of cardiovascular disease and cancer because of the inactivity they generate.
One should remain as still as possible / FALSE
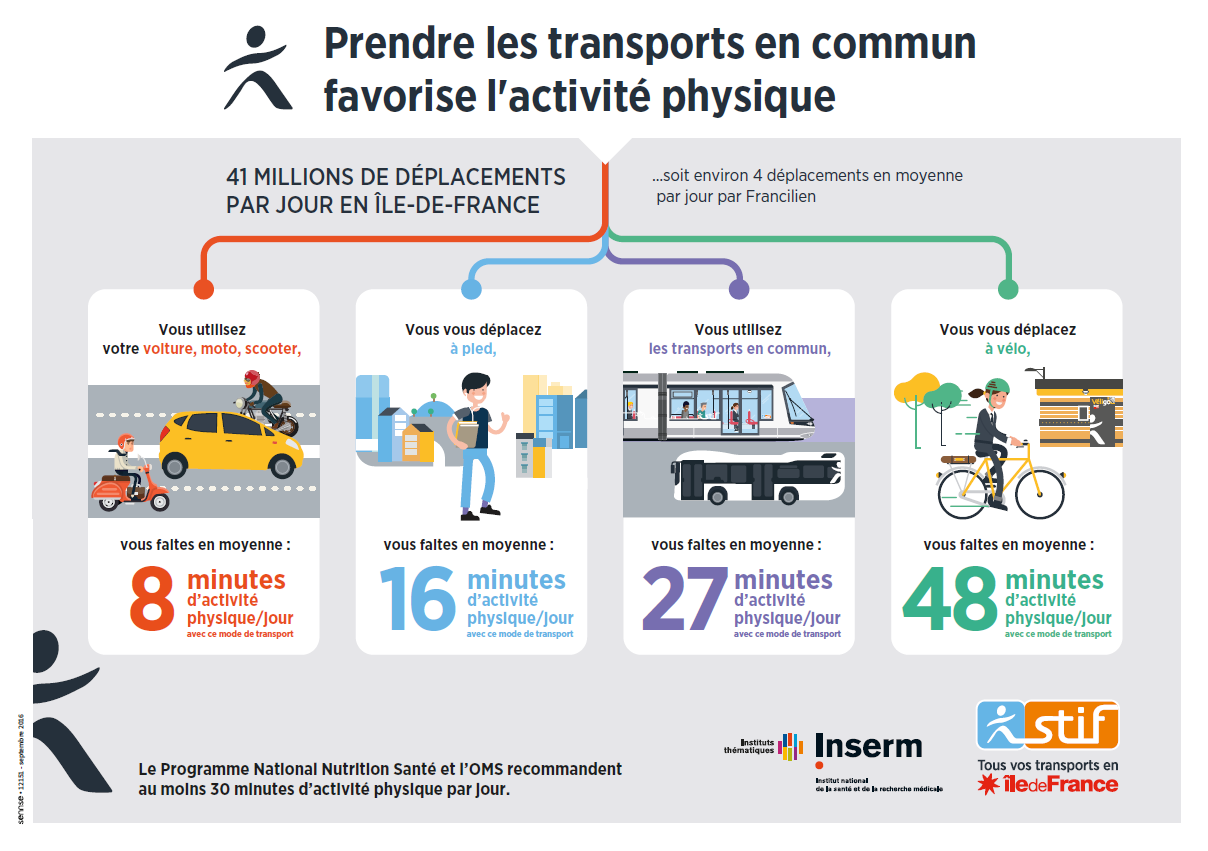
On the contrary, physical activity, which is impeded by mobility problems in people affected by these diseases, is also a remedy for maintaining one’s bone and joint capital.
What should be remembered from the IFOP survey:
How common rheumatic diseases are
A large majority of respondents (93%) have already had joint pain at least once in their lifetime. 8 out of 10 French people have even experienced it several times.
1 in 2 French people and 1 in 3 young people (18-24 years) are presently suffering (at the time of responding to the survey) from joint pain.
These figures, when compared to those for the prevalence of rheumatic diseases in Europe (one in four people has rheumatic disease), may suggest that the French are “patients” without knowing it. Most of them do not associate their bone and joint pain with the possibility of being treated for rheumatic disease.
The researchers therefore recommend speaking more and more to French people about “osteoarticular/bone and joint diseases” rather than “rheumatism.” First, because the word “diseases” gets away from the concept of being destined to have this pain. Second, because the words “osteoarticular” or “bone and joint” specifically describe the location of the problems (bones and joints), in the same manner as “cardiovascular disease” or “lung disease.”
Received ideas
8 out of 10 French people wrongly believe that rheumatic diseases are never fatal. In reality, due to the resulting inactivity, mortality is increased by 50% when walking is limited by these diseases.
The majority of respondents believe that rheumatic diseases are age-related, and cannot affect children. In reality, 4,000 children in France suffer from idiopathic juvenile arthritis.
Impact on daily life
Joint pain strongly affects the daily life of people who suffer from it. Three quarters of them mention at least one impact on the following activities: sleep, leisure activities, working life, family life, and life with spouse/partner.
These diseases have a particular impact on quality of sleep and the inability to take part in a leisure activity.
What about research?
Medical research is a major asset in combating rheumatic diseases, the leading cause of disability worldwide, and which affect more than one quarter of the European population.
Some twenty years ago, for example, collaboration between basic and clinical research enabled the discovery of innovative drugs. These are biotherapies such as anti-TNF agents, which specifically target inflammatory molecules. These discoveries revolutionised the treatment of patients with rheumatoid arthritis or spondylitis.
Also through research, some years ago a blood test to diagnose rheumatoid arthritis, anti-CCP, enabled physicians to diagnose the condition early, thereby allowing them to initiate treatment before the joints become damaged.
Many other bone and joint diseases have not yet benefited from advances in research. Inserm researchers are working to try to find new treatments. In France, highly ambitious projects are supported by the 3 bodies involved in the ECR initiative.
MIRIAD PROJECT
“MIcrobiome Research Initiative on spondyloArthritis and Dysbiosis”
THE MIRIAD project, led by Prof. Maxime Bréban, a researcher at Inserm Unit 1173, “Infection and Inflammation,” and a physician at Ambroise-Paré Hospital, Paris (AP-HP), in collaboration with INRA and the Flanders Institute of Biotechnology, Ghent (Belgium), will study the influence of environment on inflammatory rheumatic diseases and has the following specific objectives: 1) To identify a diagnostic marker, 2) To test a new therapeutic strategy that involves restoring the equilibrium of the microbiota in patients with spondylitis by administering a healthy microbiota.
ROAD PROJECT
“Research on Osteoarthritis Diseases”
The ROAD project, led by Jérôme Guicheux, Inserm Research Director in Nantes (Inserm Unit 791, “Laboratory of Osteoarticular and Dental Tissue Engineering:” LIOAD), is the first networked research project on osteoarthritis in France, bringing together the 7 best academic and clinical laboratories. It has the following objectives: 1) To classify the different types of osteoarthritis in mice, 2) To classify the types of osteoarthritis of the knee in humans, and to create the first National Bank of human osteoarthritic tissues, 3) To identify new biomarkers and specific targets, in order to develop innovative therapeutic strategies.
These two projects constitute pioneering initiatives in Europe. Microbiota and ageing are, moreover, two of the three priority cross-disciplinary research programmes in Inserm’s 2016-2020 strategic plan.
ESPOIR AND DESIR (Hope and Desire) COHORTS
Two national multicentre cohorts for rheumatoid arthritis (ESPOIR cohort) and spondylitis (DESIR cohort), in which several Inserm teams are participating, have already given rise to many discoveries regarding the risk factors for these diseases, such as smoking or poor oral hygiene. Prof. Xavier Mariette (Inserm Unit 1084) is coordinating a clinical trial in the ESPOIR cohort aimed at improving the oral status of patients suffering from rheumatoid arthritis.
Can rheumatic diseases be prevented?
In the absence of treatment, it is possible to conduct preventive action on rheumatic diseases. Developing the notion of “Joint Capital,” the capital that must be maintained for life at any cost, and particularly from childhood, is vital. This capital is essential, since once it is affected by one or other of these diseases, loss of this capital ends in inactivity, with known harmful consequences for the heart and blood vessels, among other things.
This “Bone and Joint Capital” relies on:
- Specific physical activity, that needs to be tailored for patients with a bone or joint disease.
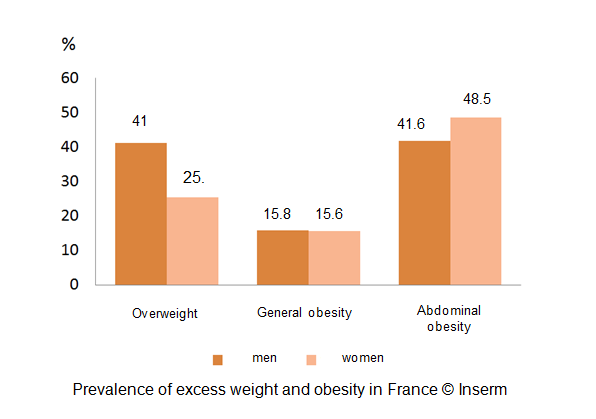
- A balanced diet, to avoid both overweight, a major risk factor for rheumatic disease, and deficiency in calcium and vitamin D, which increases the risk of osteoporosis and hence of fracture.
- Smoking cessation and good oral hygiene, to eliminate 2 demonstrated risk factors for the initiation and aggravation of rheumatoid arthritis.
- Trauma prevention programmes, from childhood/adolescence:
- Writing textbooks (junior and senior secondary school level, in Life and Earth Sciences) explaining the physiological functioning of the musculoskeletal system, and the environmental risk factors for the main bone and joint diseases, to help incorporate the concept of “Bone and Joint Capital”
- Training sports coaches in the consequences of trauma for the bones and joints (targeted warm-ups, strengthening the muscles to stabilise the joints, appropriate interruption of sports in the event of trauma, etc.)
- In older people, prevention of falls, which cause fractures in patients with osteoporosis.
A day to talk about it
World Arthritis Day (WAD) takes place on 12 October every year. On this day Inserm, Aviesan (National Alliance for Life Sciences and Health), Fondation Arthritis and the French Society for Rheumatology (SFR), 3 major bodies that fund rheumatology research in France, have joined forces to organise the
ECR 2016 (Ensemble Contre les Rhumatismes) day. Its objective will be to speak with one voice to the public and relevant politicians about the importance of supporting research on rheumatic diseases.
It will be held at the Daunou building from 10 am to 4 pm, in the form of round table discussions broadcast live on the Web and in 2 French cities.
Each theme of the “ECR 2016” day will be successively presented by a researcher and by a representative of a patient association, and followed by a discussion to enable the exchange of points of view between researchers, physicians and patients.
The programme has been prepared in very close collaboration with the patient associations, which were invited to a first meeting at Inserm to propose and select themes and speakers to meet their needs.
Further information: www.ensemblecontrelesrhumatismes.org
Email: gro.semsitamuhrselertnocelbmesne@ofni
gro.semsitamuhrselertnocelbmesne@muabnerebsicnarf
[1] Rheumatic diseases comprise all diseases of the musculoskeletal system (bones / cartilages / muscles / tendons / ligaments)